(Last Updated - 6/5/2007)
-aka Hives
-closely related to angioedema
-urticaria involves only the superficial dermis vs. angioedema which involves deeper skin layers including the sub-Q tissue
-< 6 weeks duration --> acute (usually 24-72 hrs)
-> 6 weeks duration --> chronic
-incidence increases after adolescence (highest in 3rd decade)
-Charaterizations:
-rapid-onset
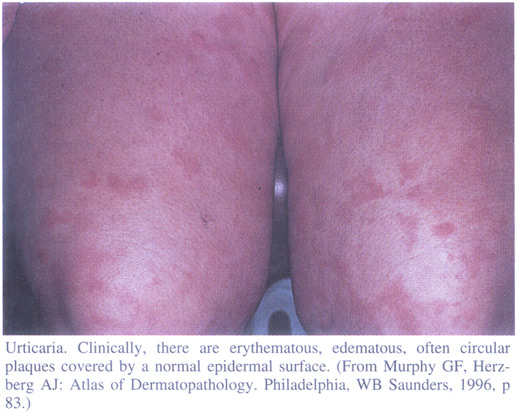
-well-circumscribed wheals w/ erythematous, raised, serpigionous borders w/ blanched centers that may coalesce to become giant wheals
-pruritic
-may involve any body area --> scalp to soles (most commonly face / extremities)
-lesions appear in crops lasting 24-72 hrs. --> old ones fade and new ones erupt (various stages)
-self-limited in nature (usually) --> unless airway management issues w/ angioedema
-direct reproduction w/ triggering stimulus
-equivocally elevated IgE level or peripheral eosinophilia
-Classification:
1) IgE-Dependent:
A) Specific Ag Sensitivity Urticaria --> pollens, foods, drugs (Ex.) Warfarin (Coumadin)), fungi, molds, Hymenoptera (bees/wasps) venom or helminths (worms)
B) Physical Urticaria --> should be distinguishable by history
I) Dermographism:
-occurs in ~1-4% of cases
-characterized by a linear wheal at the site of a brisk physical stroke along the skin
II) Cold Urticaria:
-local irritation at areas exposed to cold (Ex.) ice)
III) Solar Urticaria:
-same as above #II but with sun exposure
IV) Vibratory Urticaria:
-possible occupational relation
V) Pressure Urticaria:
-history will indicate sustained stimulus (Ex.) straps, belts or running)
VI) Cholinergic Urticaria:
-characterized by small-sized wheals (1-2 mm) surrounded by large areas of erythema
-may be precipitated by fevers, hot baths or showers
-presumedly due to increased core body temperatures
VII) Exercise-Related Urticaria:
-differentiate from cholinergic because lesions are not preceded by increased core body temperatures and wheals are conventionally-sized
2) Complement-Mediated:
A) Necrotizing Vasculitis --> immune complex disease
-more common in females
-associated with arthralgias
-characterized by an elevated ESR
-may be normo- or hypocomplementemic
-typically lasts > 72 hrs
-confirm diagnosis via skin biopsy --> fibrinoid venular necrosis
B) Serum Sickness --> immune complex disease
C) Reactions To Blood Products
3) Non-Immunologic:
A) Direct Mast Cell-Releasing Agents:
-Opiates
-Antibiotics
-Curare
-D-Tubocurarine
-Radiocontrast Media
B) Arachidonic Acid Metabolism-Altering Agents:
-Aspirin
-NSAID's
-Azo Dyes
-Benzoates
4) Idiopathic
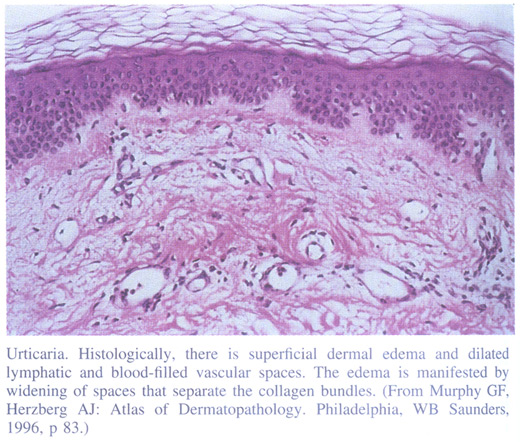
-Histology:
-collagen bundles in affected areas separate widely --> allows venule dilation
-perivenular infiltrate:
-lymphocytes, eosinophils, neutrophils, mast cells --> degradation products --> Histamine
-Treatment (In Order of Progression):
1) H1-antihistamines (Ex.) Chlorpheniramine or Diphenhydramine (Benadryl))
2) Less Sedating H1-antihistamines (Ex.) Loratadine (Claritin) or Cetirizine (Zyrtec))
3) Cyproheptadine (Periactin) or Hydroxyzine (Atarax)
4) Doxepin (Sinequan) (both H1 and H2 antihistamine)
5) Add Hydroxychloroquine (Plaquenil) or Colchicine to #3 or #4 above
6) Systemic Glucocorticoids --> last option EXCEPT in:
-pressure urticaria / vasculitic urticaria
*** Topical Glucocorticoids of no value ***
========================================================
References:
1) Harrison's Principles of Internal Medicine - 15th Edition - 2001. Chapter 310.
2) Robbins Pathologic Basis of Disease - 6th Edition - 1999. Chapter 27.